
Carly Hood, MPA, MPH
Population Health Service Fellow
Wisconsin Center for Health Equity
Health First Wisconsin
Wisconsin Division of Public Health
Madison, Wisconsin
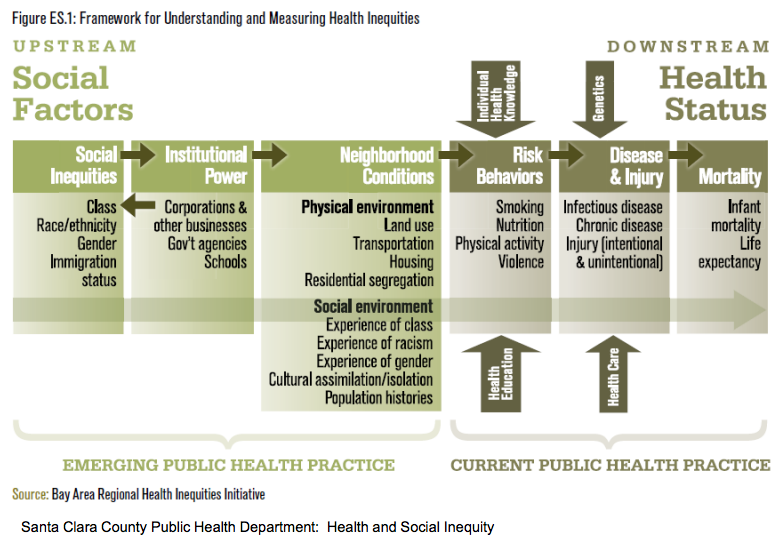
Somewhat counterintuitive and disturbing, I was surprised to
learn that we have seen a dynamic shift in where poverty in our country exists,
and today there are more poor people living in the suburbs than the cities
(reinforced by this infographic).
 This is in part the result of what’s known as the “drive
til you qualify” phenomenon whereby if you want a shorter and cheaper
commute, you have to be able to pay for it in home price (and vice versa). This
lack of regulation on housing prices and affordability, as Professor
Dunham-Jones pointed out, has led to uneven and unsustainable patterns in development
as we see them today.
This is in part the result of what’s known as the “drive
til you qualify” phenomenon whereby if you want a shorter and cheaper
commute, you have to be able to pay for it in home price (and vice versa). This
lack of regulation on housing prices and affordability, as Professor
Dunham-Jones pointed out, has led to uneven and unsustainable patterns in development
as we see them today.
But it was as she shared pictures of a case study (one from
her incredible database of 800 locales!) from my home state of Oregon that I
got to thinking…not all suburbs are created equal. She was sharing changes made
to a structure in a suburb of Portland called Lake Oswego which happens to have
the
greatest concentration of Portland-area homes worth more than $1 million.
And so it struck me: Are the people in Lake Oswego the people most in need of
retrofitting for the “public’s health?” Now I recognize that this is just one
of many examples of a suburb that is
reusing space for new purposes; some examples are found in impoverished communities,
others in more well off areas. And Professor Dunham-Jones did share stories from both ends of the spectrum. But given that lower
socioeconomic status has consistently been associated with poorer health
outcomes (which holds across the income gradient), if one of the goals of
“retrofitting suburbia” is to improve population health, wouldn’t we be more
successful at achieving this goal if our efforts were more often targeted in
areas with poor health, less community cohesion, and fewer options for safe
shared space?
There’s no doubt empty strip malls, large parking lots, and
poorly designed suburban neighborhoods are not only eye-sores, but are
contributing to our
car-dependent and chronic-disease ridden country.

But should we be looking towards those with longest
commutes, fewest parks, and/or highest rates of morbidity to consider such
beneficial transformations? And even before
we ask those questions, I’d explore just what may be occurring inside those
communities that we can’t see from the outside…Kaid Benfield, Special Counsel for Urban
Solutions at Natural Resources Defense Council, highlights, “As [suburban] properties
have declined, so have their rents, making
them affordable to small, often entrepreneurial businesses,” businesses often
owned and frequented by inner-suburb immigrant populations. Says Benfield, “The risk is that,
as we reshape these old properties with new buildings and concepts, the
replacement properties will be much more valuable than their predecessors;
indeed, that’s why new development is appealing to investors and how it is made
possible. Overall, that’s a good thing. But small businesses either
go under, unable to afford new rents, or relocate as a result. “ In housing policy, when an area is rezoned many
cities now have inclusionary
zoning policies e.g: “a percentage of
units in a new development or a substantial rehabilitation that expands an
existing building set aside affordable units in exchange for a bonus density.
The goals of the program are to create mixed income neighborhoods; produce
affordable housing for a diverse labor force; seek equitable growth of new
residents; and increase homeownership opportunities for low and moderate income
levels.” But that policy doesn’t necessarily translate to the rezoning
of small, local businesses run by lower and middle class populations.

Alas, the challenges remain—and professor Dunham-Jones spoke
eloquently to these: How do we ensure beautifying old structures isn’t pushing
out the very people who are making the only use of them? How do we even
determine if in fact retrofitting efforts ARE having an impact on health? And
finally, I’d push us to ask: are we getting at the roots of the problem? Increasingly
more and more people across the country are spending less time using services,
purchasing goods and/or enjoying public space.
America’s poor paying jobs that demand long hours, multiple shifts,
and/or too much time in transit are squeezing our middle class. An extreme
example, but one we could do well to learn a lesson from before it’s too late,
is that of China’s ghost cities, captured here
on CNN.
I see the benefits of retrofitting our suburban landscape,
and through Professor Dunham-Jones’ lecture, have learned of the amazing
structures and spaces erected, community built, economies revitalized and local
business improved through such efforts. I recognize health is not the only goal in redeveloping our suburban
landscape, and equity can’t be the sole
factor in determining repurposing projects. But that’s the lens I wear. And for
those most sick and in most in need of a louder voice, I can’t help but ask,
“How do we decide fairly which space
to retrofit?”






































{kind=link}